

Preimplantation
Genetic Testing
PGT-A
PGT-A (Preimplantation Genetic Testing for Aneuploidies) analyzes the 23 chromosome pairs of the embryo before transfer. Only genetically intact embryos are transferred, improving implantation and reducing miscarriage risk.

PGT-A (Preimplantation Genetic Testing for Aneuploidies) is a study that analyzes the 23 chromosome pairs of the embryo before transferring it to the uterus. It allows us to identify which embryos have chromosomal integrity and discard those carrying numerical alterations (aneuploidies) that generally prevent development or cause miscarriages.
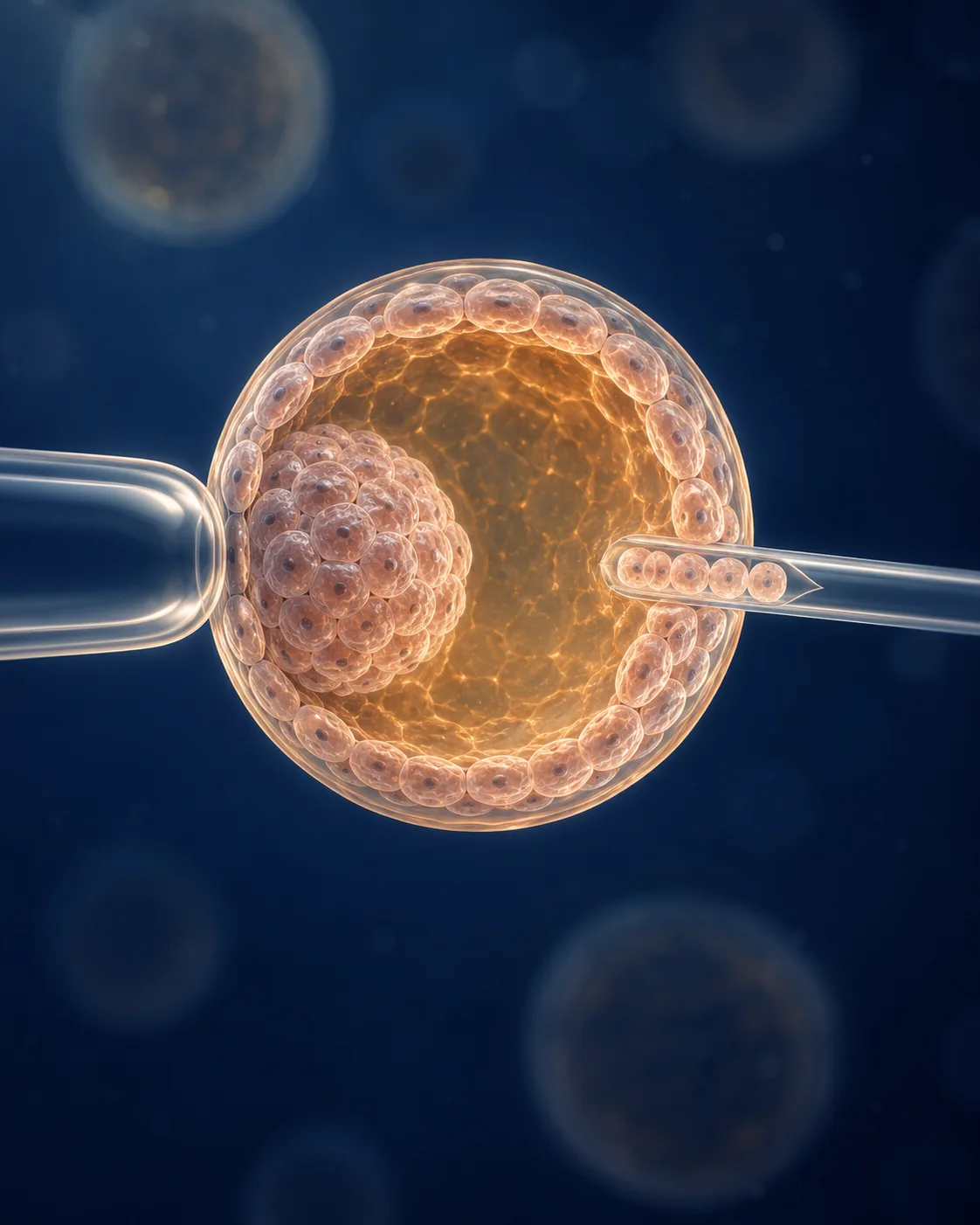
It is applied within an IVF cycle. After embryo culture to day 5 or 6, a small sample is taken from the trophectoderm (the outer layer that will form the placenta, not the baby) and sent to the genetics lab for analysis with NGS (Next Generation Sequencing) technology.
The result puts key information on the table: which embryos have real potential to implant and result in a healthy baby. Clinical decisions with data, not blind ones.
- 0 pairs Chromosomes analyzed
- 0% Diagnostic precision
- Up to 0% Miscarriage risk reduction
Why it changes the treatment outcome
-
Only intact embryos are transferred
The lab identifies the embryos that have the correct number of chromosomes in each pair. Those are the ones with real capacity to implant and develop until birth.
-
Reduces miscarriage risk
One of the most common causes of early miscarriage is chromosomal alterations in the embryo. By transferring only fit embryos, that probability drops significantly.
-
Shortens the path to an ongoing pregnancy
Fewer failed transfers, fewer early losses, less time wasted. For profiles with advanced reproductive age or previous losses, this translates into reaching the baby sooner.
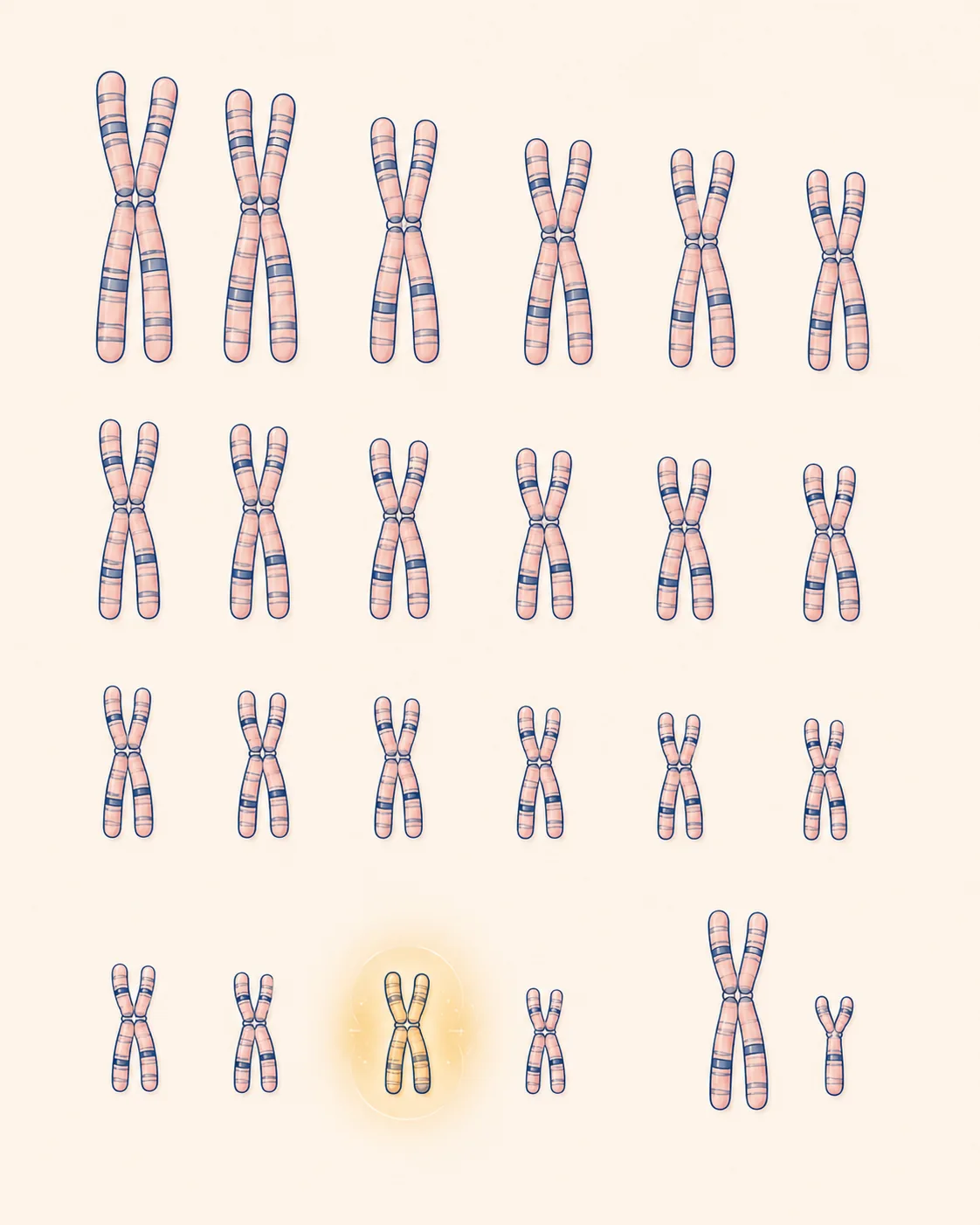
The 23 pairs, read before transfer
A healthy human embryo has 46 chromosomes organized in 23 pairs: 22 autosomes plus the sex pair (XX or XY). When there is an extra or missing chromosome in any pair, the embryo presents an aneuploidy. Most do not implant, the implantation is interrupted by early miscarriage, or the pregnancy evolves with severe syndromes.
PGT-A reads those 46 chromosomes with NGS technology, one of the most precise genetic techniques available today. The result is clear: each embryo is classified as euploid (intact chromosomes, fit to transfer), aneuploid (with alteration, not fit), or mosaic (intermediate result, evaluated case by case).
That transforms embryo transfer from a probabilistic bet into an informed decision backed by data.
Profiles where PGT-A adds real clinical value
-
Advanced reproductive age
From age 37 in women and 38 in men, the probability of aneuploidies rises. PGT-A is a standard clinical indication from that age.
-
Recurrent pregnancy loss
When there is a history of two or more miscarriages, especially in the first trimester, PGT-A helps avoid new losses due to chromosomal causes.
-
Previous implantation failures
After two or more transfers of morphologically good embryos without success, genetic testing identifies whether there is a chromosomal factor not detected before.
-
Male factor with DNA fragmentation
When sperm shows high DNA fragmentation, aneuploidy risk rises. PGT-A confirms which embryos came out genetically fit.
-
Family history of chromosomal alterations
When one of the partners carries a balanced translocation or has relevant family history, the study is practically indispensable.
-
Single healthy pregnancy goal
By identifying the embryo with the best potential, only one is transferred with high confidence. That reduces multiple pregnancies and their associated complications.
Your path is unique. So is your plan.
We design a protocol tailored to you after understanding your story and your previous tests. No generic diagnoses or protocols.
Three stages integrated into the IVF cycle
1. Culture to blastocyst. Embryos generated by IVF (with or without ICSI/PICSI) are cultured under controlled conditions until day 5 or 6 of development. That is when the embryo reaches the blastocyst stage and can be biopsied without affecting its viability.
2. Trophectoderm biopsy. The embryologist takes 3 to 5 cells from the outer layer of the embryo (the trophectoderm, which will form the placenta, not the baby). It is a minimally invasive procedure, widely clinically validated, with no impact on subsequent development.
3. Genetic analysis and transfer. The sample is sent to the genetics lab for NGS analysis. Meanwhile, embryos are vitrified. When results arrive, one or two euploid embryos are transferred in a later cycle, with optimal endometrial synchronization.

Chromosomal alterations PGT-A identifies
-
Trisomy 21 (Down Syndrome)
Extra chromosome 21. It is the best-known trisomy and one of the classic indications for PGT-A in advanced maternal age.
-
Trisomy 18 (Edwards Syndrome)
Extra chromosome 18. Causes multiple severe anomalies and, in most cases, early pregnancy loss.
-
Trisomy 13 (Patau Syndrome)
Extra chromosome 13. Like Edwards, usually incompatible with life or with severe neurological development.
-
Klinefelter Syndrome (XXY)
An extra X chromosome in males. Affects testicular development and fertility. PGT-A identifies it before transfer.
-
Turner Syndrome (X0)
Missing X chromosome in females. Associated with short stature, cardiac issues, and ovarian dysgenesis.
-
Other aneuploidies
Triple X (XXX), Jacobs (XYY) and aneuploidies in any of the other chromosome pairs. The analysis covers all 23 pairs.
PGT-A within the TripleMed™ model
PGT-A is not applied as an isolated study. At Ingenes it is integrated into the IVF cycle within the TripleMed™ model, which combines reproductive medicine, genetic and regenerative medicine, and metabolic medicine in a single personalized plan.
That means your case is reviewed by a multidisciplinary team: reproductive physician, embryologist, geneticist, regenerative specialist, and metabolic specialist. Every decision about biopsy, transfer, or adding other genetic studies (PGT-M, Clarix™) is made with shared clinical criteria, not by default.
We work with proprietary NGS technology, an in-house embryology lab, and personalized protocols after more than 20 years of experience in high complexity. That integration is what turns a single genetic analysis into one piece of a plan aimed at an ongoing pregnancy.

Frequently asked questions about PGT-A
What is the difference between PGT-A and PGT-M?
PGT-A detects aneuploidies (alterations in the number of chromosomes, like Down or Edwards). PGT-M looks for a specific genetic mutation linked to a known hereditary disease in the family (cystic fibrosis, sickle cell anemia, muscular dystrophy, etc.). They are different studies with different indications and can be combined in the same cycle if the case justifies it.
Does the biopsy harm the embryo?
No. The biopsy is taken from the trophectoderm (the outer layer that gives rise to the placenta), not from the inner cell mass that will form the baby. It is a widely clinically validated procedure, with thousands of healthy babies born after PGT-A worldwide.
What happens to aneuploid embryos?
They are embryos that do not have real capacity to develop to term. They generally do not implant or result in early miscarriage. The decision on what to do with them is discussed with the couple and their wishes are respected within the current legal framework.
What is a 'mosaic' embryo?
An embryo whose biopsy shows a mixture of euploid and aneuploid cells. Its evolution is variable: some result in healthy pregnancies, others do not. Each mosaic is evaluated based on its percentage and the chromosome affected to decide whether to transfer it. The team explains the risk/benefit balance.
How long does the result take?
Between 2 and 3 weeks from the biopsy. That is why embryos are vitrified while waiting for the result, and the transfer is performed in a later cycle (deferred transfer). That strategy also improves endometrial receptivity.
Does it guarantee a healthy baby?
No. PGT-A analyzes numerical chromosomal alterations, not all possible genetic conditions. That is why it is always complemented with standard prenatal follow-up (ultrasounds, Clarix™, amniocentesis if applicable). What it does do is significantly reduce the risks linked to common aneuploidies.
How much does adding PGT-A to the cycle cost?
It is an additional cost to the IVF cycle, depending on the number of embryos biopsied. We discuss it in detail at the First Consultation or during cycle planning, with concrete numbers based on your case.
Can PGT-A improve the odds in your case?
Genetic testing does not apply to every treatment. At the First Consultation we review your clinical history and tell you whether it adds real value to your plan or whether it would be unnecessary spending.
Contact us