

Artificial
Insemination
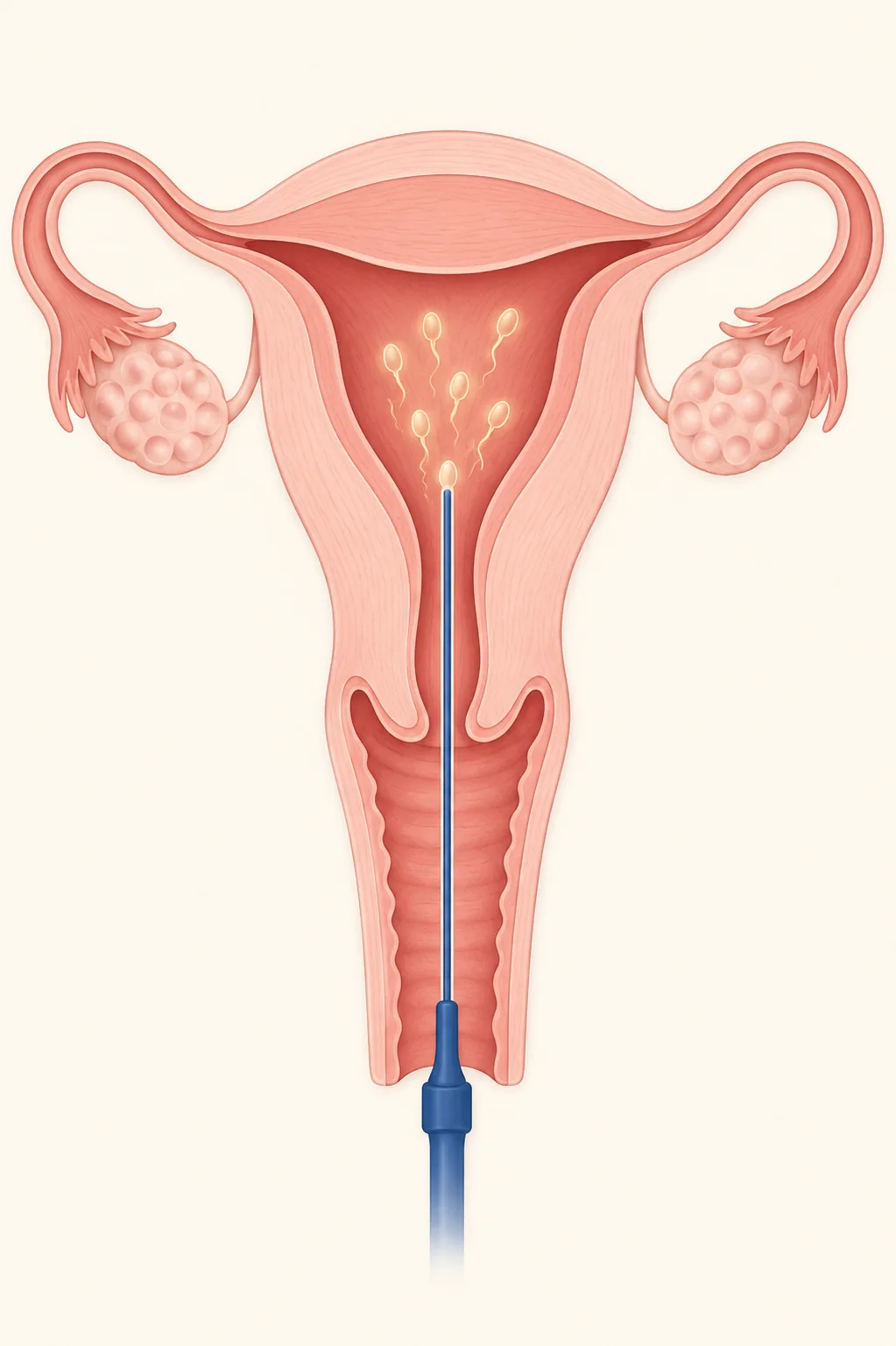
Artificial Insemination or Intrauterine Insemination (IUI) is the most common low complexity technique. We capacitate sperm in the lab and place it inside the uterus on the most fertile day of the cycle. Minimal invasiveness, first step of the journey.

Artificial Insemination or Intrauterine Insemination (IUI) is the most common low complexity assisted reproduction technique. Sperm is processed in the lab (sperm capacitation) to concentrate the highest-quality cells, and then placed directly inside the uterus on the most fertile day of the cycle, right before ovulation.
Everything else happens inside the body: fertilization, embryo development, implantation. The lab does not participate in fertilization, it only prepares the sample and times the exact moment.
It is an outpatient procedure, painless and quick. The couple walks in, the insemination is done in a few minutes, and they walk out. No anesthesia, no hospitalization, no recovery.
- 0-20% Success per cycle (under 35)
- 0-6 Cycles before escalating
- 0-3 wk Total cycle duration
Three advantages of Artificial Insemination
-
Minimally invasive
The procedure takes a few minutes, is done with a thin catheter, and requires no anesthesia. No hospitalization, no recovery. You go back to your routine the same day.
-
Capacitated sperm
The sperm sample is processed in the lab to concentrate motile sperm and discard non-viable ones. That raises the effective quality of the sperm placed in the uterus.
-
The body does the work
Fertilization happens naturally inside the reproductive system. It is the option closest to a spontaneous conception, with the extra of perfect timing and better sperm quality.
A simple technique for clinically appropriate cases
Artificial Insemination requires three biological conditions that your team confirms in the initial diagnosis: patent fallopian tubes, functional ovulation (spontaneous or induced with light medication), and a sperm sample with sufficient quality after capacitation.
When those three are met and the woman is under 35 with no other aggravating diagnoses, insemination is the logical first step. For more complex profiles, the indication shifts and we go directly to IVF without losing biological time.
Candidate profiles for Artificial Insemination
-
Mild male factor
Slightly reduced concentration or motility in the semen analysis. Sperm capacitation improves the sample to functional levels.
-
Single women
With donor sperm (in-house or international bank), insemination is the simplest and least invasive path for a single woman who wants to become a mother.
-
Female couples
With donor sperm, insemination allows one of the partners to carry the pregnancy from the start of the process, with minimal clinical intervention.
-
Unexplained infertility
When studies show no identifiable factor, insemination adds probability by concentrating the sperm on the exact fertile day.
-
Cervical issues
When cervical mucus is hostile or the cervix makes sperm passage difficult, insemination bypasses it by placing sperm directly in the uterus.
-
Mild anovulation or irregular cycles
With controlled ovarian stimulation we induce regular ovulation and sync it with the insemination to maximize timing.
Your path is unique. So is your plan.
We design a protocol tailored to you after understanding your story and your previous tests. No generic diagnoses or protocols.
Four steps in a 2 to 3 week cycle
1. Initial diagnosis. We confirm with semen analysis, hormonal profile, and ultrasound that your case is a candidate. Without this step, no cycle starts.
2. Light ovarian stimulation. Oral or mild injectable medication to ensure ovulation. We run follow-up ultrasounds (3 to 4 checks) to identify the exact day of the ovulatory peak.
3. Sperm capacitation. On insemination day, the sperm sample is processed in the lab (swim-up or gradient techniques) to separate the best-quality sperm and discard the rest.
4. Insemination. The physician introduces a thin catheter through the cervix and deposits the capacitated sperm directly inside the uterus. It lasts a few minutes, with no anesthesia and no significant pain. The patient can walk out.
Two weeks later a blood pregnancy test is done. If positive, obstetric follow-up begins. If negative, the team evaluates with you whether to run another cycle or reshape the plan.


The moment to move to IVF
Artificial Insemination has a clear ceiling. After 3 to 6 cycles without achieving pregnancy, the chances of success in further attempts drop significantly. Insisting beyond that range without reshaping the plan usually means losing biological time, especially if the woman is over 35.
In those cases the indication is to escalate to In Vitro Fertilization (with or without ICSI/PICSI). It is neither a step back nor bad news: it is the honest reading of the diagnosis. We tell you that openly in the follow-up consultation.
See High Complexity
Frequently asked questions about Artificial Insemination
What is the success rate of Artificial Insemination?
Between 10% and 20% per cycle in women under 35 without aggravating factors. The rate varies based on age, sperm quality, the cause of the diagnosis, and the response to stimulation. That is why 3 to 6 cycles are planned as the window to evaluate results.
Is it painful?
No. It is an outpatient procedure similar to a Pap smear. A thin catheter is introduced through the cervix and the sperm is deposited. Some patients report mild discomfort, comparable to a minor menstrual cramp, that passes in minutes.
How long does a full cycle last?
Between 2 and 3 weeks from the start of stimulation to insemination, plus 2 weeks waiting until the pregnancy test. In total, the cycle takes about one calendar month.
How many attempts should we do before moving to IVF?
The standard is 3 to 6 cycles. After that range, chances drop significantly. If pregnancy was not achieved, the team evaluates moving to IVF. Insisting further without reshaping usually means losing biological time.
Does it work with donor sperm?
Yes. Artificial Insemination with donor sperm (in-house bank or international bank) is the standard path for single women and female couples. The procedure is exactly the same, only the origin of the sample changes.
What are the risks?
Risks are low. There may be a minimal risk of local infection (very rare because we work with a capacitated and sterile sample) or multiple pregnancy if ovarian stimulation was used (controlled with strict ultrasound monitoring). We discuss it at the First Consultation.
Do I need bed rest afterward?
It is not mandatory. We recommend 10 to 15 minutes of rest in the consulting room after the procedure, and then you can go back to your routine. Some physicians suggest avoiding intense exercise that same day, but normal life continues as usual.
Is Artificial Insemination the right path for you?
We define it with a clear diagnosis, not by default. We start at the First Consultation to see if your case has real chances with this technique.
Contact us