

Endometriosis and Fertility: A Simple Guide

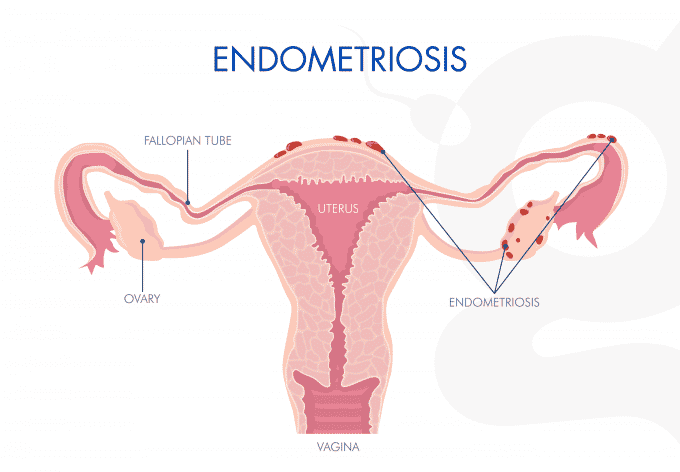
Endometriosis occurs when the tissue that normally lines the inside of the uterus appears elsewhere, such as on the ovaries or pelvic cavity. This abnormal growth can cause pelvic organs to stick together, leading to pain and impairing fertility.
The condition can block the fallopian tubes or reduce ovarian reserve, making conception more difficult. For those wishing to become parents, In Vitro Fertilization (IVF) is often the best option. In IVF, eggs are fertilized in the lab and healthy embryos are transferred to the uterus.
What is endometriosis and how does it affect your fertility?
Endometriosis occurs when tissue similar to the uterine lining grows outside the uterus, on the ovaries, fallopian tubes, or peritoneum. Each menstrual cycle, this tissue bleeds without an exit, causing inflammation, scarring (adhesions), and pain. These adhesions can alter pelvic anatomy, block the tubes, and hinder ovulation, lowering the chances of natural conception.
Studies show endometriosis can reduce both egg quality and quantity, as well as affect ovarian reserve markers like anti-Müllerian hormone (AMH). Early diagnosis and treatment improve outcomes. More details at Endometriosis: What is it and How Does it Impact Your Fertility?
How to identify if you have endometriosis
The most common symptoms are:
- Severe menstrual pain that limits daily activities.
- Chronic pelvic pain, sometimes radiating to the back or legs.
- Pain during intercourse.
- Irregular bleeding or spotting between periods.
- Fatigue and digestive issues like bloating or diarrhea.
Diagnosis usually starts with a pelvic ultrasound, preferably transvaginal, and is confirmed by laparoscopy. At Ingenes, we choose ultrasound first to detect endometriomas, adhesions, and deep lesions with less invasiveness.
Treatments to improve fertility in endometriosis
Initial management may include anti-inflammatory medications for pain, hormonal therapy (e.g., GnRH agonists), and surgery to remove adhesions and restore pelvic anatomy. If pregnancy is the goal, Assisted Reproductive Technologies (ART) are often recommended post-surgery.
IVF remains the most effective option in moderate to severe cases. Controlled ovarian stimulation protocols aim to retrieve multiple oocytes (8–15 mL of follicular fluid per follicle). Before starting, consult with a reproductive endocrinologist. Avoid self-medication.
Lifestyle changes that support your fertility
A diet rich in omega-3 fatty acids and antioxidants (fruits, vegetables) and low in red meat helps control inflammation. Regular low-impact exercise (yoga, swimming) improves pelvic circulation and relieves pain.
Maintain a healthy BMI (18.5–24.9 kg/m²), avoid smoking, and limit alcohol. Stress-management techniques also benefit reproductive health.
Frequently Asked Questions About Endometriosis and Fertility
1. How Does Endometriosis Stage Affect My Chances of Pregnancy?
The American Society for Reproductive Medicine (ASRM) classification ranges from I to IV. Stages I–II have higher natural fertility, while stages III–IV involve more adhesions and ovarian damage. Each case is unique: large endometriomas (>3 cm) may require surgery or ART.
2. What Are the Risks of Surgery Before Trying to Conceive?
Laparoscopy removes lesions and improves tubal mobility but can reduce ovarian reserve and create new adhesions. Discuss with a specialist to balance benefits and risks based on your reserve and goals.
3. What Is the IVF Success Rate in Endometriosis?
It depends on age and severity. For women under 35 with mild to moderate endometriosis, the clinical pregnancy rate per cycle is around 40–50%. In severe cases, rates are lower, but combining surgery with personalized protocols improves outcomes.
4. Can Endometriosis or Its Progression Be Prevented?
There’s no sure way to prevent it, but early detection and hormonal treatment can slow ectopic tissue growth. Maintaining an anti-inflammatory lifestyle (diet, exercise, stress management) helps control symptoms.
If you experience severe pelvic pain or menstrual irregularities, see your gynecologist as soon as possible for timely evaluation.
Sources
- American Society for Reproductive Medicine. (2012). Revised American Society for Reproductive Medicine classification of endometriosis: 1996. Fertility and Sterility, 67(5), 817–821. doi.org/10.1016/S0015-0282(16)62896-3
- National Institute of Child Health and Human Development. (2020). Endometriosis. MedlinePlus. https://medlineplus.gov/endometriosis.html
- Giudice, L. C. (2010). Clinical practice. Endometriosis. The New England Journal of Medicine, 362(25), 2389–2398. doi.org/10.1056/NEJMcp1000274
- Leonardi, M., et al. (2018). Transvaginal ultrasound mapping of deep endometriosis. Human Reproduction Update, 24(2), 234–250. doi.org/10.1093/humupd/dmx042
We understand how challenging this journey can be. You are not alone: seek professional support and consider guidance from a fertility specialist to increase your chances of achieving that long-awaited pregnancy.


